


What the Diamond Princess tells us about NYC in Spring 2020
Connecting the defining events of early 2020
by Dr Todd Kenyon
In our continuing effort [part 1 of series] to use relatively simple arguments that allow for an honest look at the accuracy of the prevailing narrative, we turn next to analyse what happened on the Diamond Princess (DP) cruise ship during its reported “outbreak” of Covid.

Here we intend to examine how this purported “worst case” scenario actually unfolded on the ship. Did the Covid case and death numbers on the DP add up to a “novel deadly virus” that required “shutting down the world”? How does what happened on the DP compare to early hotspots like New York City, and what can we learn from the comparison?
The first wave of putative Covid deaths in Spring 2020 demonstrated extremely unusual characteristics in some areas - including New York City and Bergamo, Italy. Excess mortality exploded overnight at precisely the time restrictions were implemented, whereas there was no sign of anything unusual immediately prior. The mortality peaks rocketed to unprecedented levels of excess mortality and then quickly subsided. As has been observed in relation to Northern Italy and New York City, the shape and severity of the mortality curves do not appear as one would expect from a naturally spreading virus. Did something other than a novel virus drive these steep first waves, and if so how can we estimate the contribution of the virus?

As it turns out, there was an event that serves as an isolated “laboratory,” and therefore can provide clues to the true severity of the SARS-CoV-2 virus. The Diamond Princess cruise ship departed Japan on January 20, 2020. Five days later a passenger disembarked, later became ill and tested positive for SARS-CoV-2 infection. On board this ship were 3,711 persons, of which 2,666 were passengers (median age of 69) and 1,045 were crew (median age of 36). Nearly half (48%) of the passengers were said to have underlying disease(s). Passengers and crew began testing positive with some becoming ill, but the passengers were not quarantined in their cabins until Feb 5. Until that time they had been engaging in a variety of typical social activities including shows, buffets and dances. Once quarantined (confined to cabins), most passengers shared cabins with 1 to 3 other passengers. Cabins used unfiltered ventilation and the crew continued their duties and mixed with passengers. Evacuation began in mid February and was completed by March 1.
A total of 712 individuals (19%) tested positive via PCR, and as many as 14 passengers were said to have died, though there are differing opinions as to how many of these deaths should be attributed to Covid. Except for one person in their late 60s, all deaths occurred in those over 70. Not one crew member died. Half of the deaths occurred several weeks after leaving the ship, so it is unclear if they actually died from infections caught onboard. Three ill passengers were given an experimental treatment of Remdesivir once hospitalised on shore; apparently all survived.


The Diamond Princess was termed a “virus mill” by one expert while another remarked that cruise ships are perfect environments for the propagation and spread of viruses. The quarantine procedures inflicted much duress on an already frail passenger base and may have done more harm than good. There was panic and confusion both among passengers and crew, and densely packed passengers sharing unfiltered ventilation were only allowed out of cabins every few days for an hour. Meanwhile the crew continued to prepare meals and mix with passengers, but otherwise were kept confined below the waterline in their cramped multi-resident quarters. Some passengers ignored the quarantine entirely. The so-called “Red Dawn” email discussions among government researchers in early 2020 described the DP as a “quarantine nightmare.” The DP was also termed by this group as representative of a large elderly care home (passengers). Based on all these observations, the DP event should provide a nearly worst case scenario for the first wave of Covid. The question is, how did New York City (NYC) fare versus this “worst case”, and what can we learn from the comparison?
We can start by looking at the infection rate on the DP: 25% of those over 60 and 9% of those under 60 were reportedly infected. On the DP, the case fatality rate (CFR) for those over 60 was 2.6%. This assumes that all 14 deaths of passengers were caused by a Covid-19 infection contracted while on the DP. On the other hand, the CFR for those under 60 years of age was 0.0%, since none in this age bracket died.

As may be seen from Figure 4, the DP data indicates that even in this population (which was heavily weighted towards vulnerable older individuals), the severity of the outbreak was mild. Furthermore, the virus was not lethal to younger, healthy individuals, not even when they were confined in a “virus mill” with the supposedly most virulent Wuhan variant. The 1,045 crew members, confined in tight quarters with no fresh air when not serving passengers, suffered no ill effects from this supposedly novel deadly virus. This alone should have influenced public policy globally, in which case much suffering would undoubtedly have been avoided. PANDA began writing about this shortly after the data was available in 2020, as did others. Still, let’s examine what happens if we compare the Diamond Princess event with New York City’s terrible first wave. As always, the goal here is to be roughly right rather than precisely wrong.
In New York City, approximately 15% of the city’s 8.77 million people are over 65, for a total of 1.3 million in this age category. If, as on the DP, 25% of them were infected, it would result in 328,000 cases of Covid. Using the estimated CFR of 2.6% as estimated from the DP data, we should expect a maximum of 8,550 Covid deaths among those over 65. Although no one died on the DP who was under 65, to establish an upper limit of mortality in NYC, we can use an IFR of 0.035% for those under 60. Assuming that 20% of the 7.45 million people living in NYC who are under 60 contracted Covid, this would have resulted in 522 deaths. This indicates that if NYC was a giant floating "Diamond Princess" cruise ship, the worst case mortality would have been 9,073 Covid deaths over 4-8 weeks (deaths on the DP were counted out to about 8 weeks past the first case).
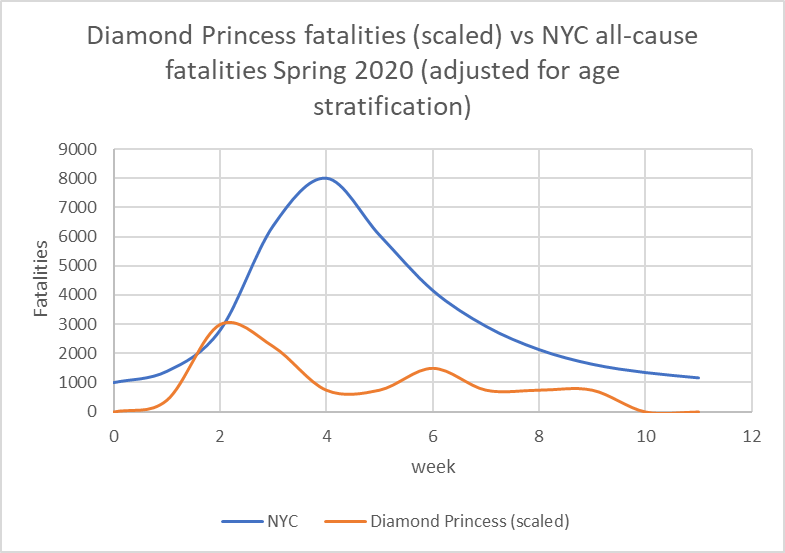
Total deaths (all causes) in NYC from week 12 to week 20 of 2020 amounted to about 38,000. This is almost four times worse than the scaled DP fatalities. According to the CDC, the CFR of Covid for those over 64 during this “first wave” in NYC was 28% (13,798 deaths, 49,124 cases). Conversely, on the Diamond Princess, even if we count all deaths as 70+, the CFR maxes out at 4.9% (14 deaths, 288 cases). While one can argue whether the respective durations of exposure are comparable, a locked down New York City should have fared much better than a confined cruise ship. Yet, amazingly, the CFR on the DP for those under 65 was precisely zero, while in NYC the CFR for those 45 to 64 was 5.7% - worse than that for those over 70 on the DP, despite it being a “virus mill quarantine nightmare”. As an additional comparison we can look at fatality data from Sweden, the country that famously did not lock down. Sweden’s first wave is barely noticeable versus NYC and clearly appears less severe than what transpired on the DP (Fig. 6).

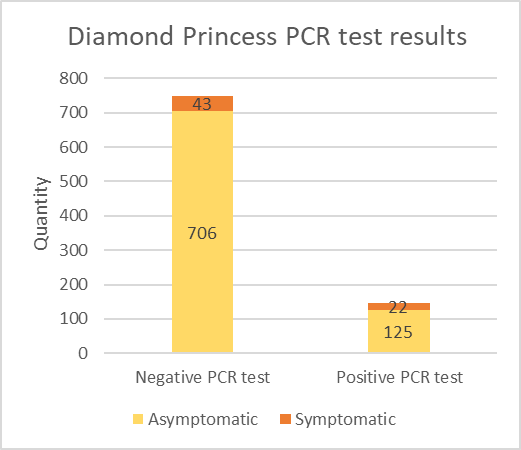
In addition, there are several factors which likely make the DP outbreak look worse than it really was. First, PCR test data taken in mid February indicate that more than half of the “positive” cases had a Cycle Threshold value greater than 30. More than half of those testing positive were asymptomatic. So the true infection rate may have been significantly less than reported. Second, it is unclear if all 14 deceased passengers died as a result of a Covid infection contracted while on board the ship.
Furthermore, the examination of 900 swab samples taken onboard the DP in mid February, indicates no correlation between Ct value of positive tests, symptomatic vs asymptomatic, or even symptoms vs positive tests. Clearly this sheds some doubt on whether those specimens considered positive really were of live infections, and whether those with symptoms (but testing negative) were actually suffering from Covid-19. In a documentary with footage largely sourced from passenger and crew cell phones, not a single person appeared ill, including some passengers evacuated to hospitals.

In conclusion, we believe that the Covid outbreak on the Diamond Princess cruise ship, the supposed “worst case virus mill,” looks mild in isolation, and it looks very mild when compared to the first wave in New York City and elsewhere (e.g., Northern Italy). Testing data from the Diamond Princess arguably indicates that the severity may well have been even milder than generally believed, and clearly was of no danger to the non-elderly.
The Diamond Princess event should have demonstrated to officials early on that this was not a particularly dangerous virus to the broad population, and that it certainly did not justify unprecedented draconian measures on a population-wide basis.
Second, it is clear from the above discussion that something else beyond Covid or the spread of a respiratory virus was responsible for a significant majority of the “first-wave” excess deaths in NYC.
Third, more likely causes of the unprecedented excess mortality in NYC need to be considered, including iatrogenic harms, psychological effects, neglect, panic stoked by constant media propaganda, ill-advised use of ventilators and sedatives, and policies relating to residents in care homes. If these were indeed the causes behind the excess in deaths in NYC in early 2020, a tragic proportion of the deaths were avoidable.
This article forms part of PANDA’s ongoing inquiry into the drivers of excess deaths. Please consider supporting PANDA’s independent insights with a donation.
And yet, they will continue to ignore the evidence and denigrate those that highlight it. And, the masses won't bat an eyelid.
It is quite interesting that remdesivir would already have leapt over the chloroquines by this stage of the plandemonium given that it was an orphaned good-for-nothing drug, and the chloroquines were supported by research going back to 2003.