


How many lives were actually saved by Covid vaccines?
Digging deeper into the data
by Thomas Verduyn
In a previous article of this series titled, It is impossible that the vaccines saved 14 million lives in 2021, we used various published information concerning the fatality rates of Covid to establish that it is utterly impossible for the vaccines to have prevented 14 million Covid deaths. We then used Pfizer’s own clinical trial results to show that the upper limit of Covid deaths prevented by the vaccine rollout was probably just shy of 74,000. As promised, we return to this topic with the goal of digging a little deeper into the data to see how close to this upper limit the real number might be.

It is appropriate to begin by explaining why we said that 73,384 is the upper limit. It will be recalled that this number was arrived at by assuming that all 4.5 billion people reported to have been given a Covid vaccine during 2021 received the Pfizer shot. But not everyone received this brand. Nor did everyone receive the two doses recommended by Pfizer. More to the point, the shots produced by the other manufacturers are generally considered to be less effective. Although the Moderna shot is typically thought to have a vaccine effectiveness (VE) on par with that of the Pfizer shot, the shots produced by Johnson & Johnson or Novavax have not fared as well in the clinical trials. Also, there is some question about how reliable the data from these trials might actually be. In any case, by applying Pfizer’s data to the entire cohort, we have overestimated the number of Covid deaths that were prevented. The true number should be less than 74,000.
The second reason is that “there is a gradual decline in vaccine efficacy,” as Pfizer testified in its six-month report. Sometimes that efficacy has gone to zero within only a few months. Naturally, since not every vaccinated person is challenged by the virus at the perfect time after their injection, it follows that some might experience the sad reality of an injection with zero efficacy.
So, how close to this upper limit did the vaccines actually come? To answer this question it is necessary to look at one of the bigger problems involved in calculating the effectiveness of the Covid vaccines. The problem is that a significant number of people (over and above what was expected based on background rates of Covid cases in the local community) became infected with Covid during the first week or two after they were injected; notably these additional cases were typically ignored in the calculations of VE.
We begin by looking at the extra infections. A study done in the UK, and involving more than one million participants, found that an almost unimaginable 33.8% of vaccinees reported Covid-like symptoms in that first week after injection. Not all of these symptoms were indicative of a Covid case, of course, but the conclusion in that study was that “symptoms cannot per se be differentiated from Covid-19 with clinical robustness.” In other words, a full one third of people getting the shot suffered (within a single week) the exact same symptoms that they were seeking to avoid. Bad as this is, however, we are not here discussing side effects. Rather, we are seeking to determine if the shots prevented any Covid deaths.
Naturally, some people who took the Covid shot would have fallen ill whether they were vaccinated or not, and others might have had similar symptoms without actually being infected with the SARS-CoV-2 virus that causes Covid. But given that 33.8% of people receiving the injections ended up with Covid-like symptoms, it is quite plausible that some developed Covid who otherwise would not have. The real question is, how many? Unfortunately, this study was not designed to answer the question as to how frequent Covid infections were after vaccination, and their data is not robust enough to provide even an estimate. For instance, only a tiny fraction (<4%) of those developing symptoms actually performed a test, and the conclusion of the article is that it was not possible to develop a method of distinguishing (based on symptoms alone) between vaccine-induced symptoms and those caused by infection.
It will be recalled from a previous article in this series that Pfizer claimed their shots prevented 154 symptomatic cases of Covid for every 21,720 people given the product. Thus, if the percentage of extra people infected with symptomatic Covid in the first week after receiving the injection is as small as 0.7%, then the Pfizer shot loses all of its stated benefit entirely. At that point it becomes functionally irrelevant whether or not VE wanes with time. Of course, if the Pfizer shot increased the number of people contracting Covid in the first week by more than 0.7% (as the above study strongly implies it does), it has a negative benefit, and may have increased the number of Covid deaths.
It is not our intent to discredit the vaccine rollout on account of only one study. Have other studies verified that a significant wave of Covid happens in the first week or two after receiving a Covid shot? Certainly—the effect is well documented. Another UK study, for example, found that “participants aged 80 years and older vaccinated with BNT162b2 … had a higher odds of testing positive for Covid-19 in the first nine days after vaccination. … Vaccine effectiveness was therefore compared with the baseline post-vaccination period.” In other words, on account of all the extra infections during the first nine days, they excluded this period in their calculation of effectiveness.
Likewise, an article in the BMJ affirmed that there has been “a genuine increased risk of contracting infection post vaccination,” especially in the first two weeks. It hardly bears mentioning that if the Covid shot increases the odds of being infected, even if from infections that occurred during the first fourteen days, it shouldn’t qualify as a ‘vaccine’. According to the Britannica, “a vaccine … is administered primarily to prevent disease.”
What about the use of booster shots to ‘top up immunity’? It has been observed that booster shots also cause an immediate increase in infections. For instance, a study of 1.2 million people in Israel attempted to compare the effectiveness of dose 3 with dose 4. To do so, they defined an ‘internal control group’ as the period of time between day 3 and day 8 after the fourth dose. They found that those in this ‘control group’ were more than twice as likely to get infected with Covid, and almost three times as likely to experience ‘severe Covid’ than those monitored after the eighth day. Similarly, a study of 50,000 staff working in Ohio clinics found that “the higher the number of vaccines received, the higher the risk of contracting Covid-19.”
This effect of increased infections during the first two weeks after receiving the Covid experimental shots is so well established that news media outlets have reported on disastrous consequences of this effect [ref, ref, ref], and medical groups have written articles about it.
The significance of the fact that the injections caused an increase in infections during the first week or two can hardly be overstated. How so? As was hinted at above, the significance lies in the fact that most studies that looked at vaccine efficacy assumed that it took at least one week for the vaccine to take effect. As a result, all the people that contracted Covid shortly after receiving the injection were typically classified as unvaccinated.
If the injections cause a noticeable wave of infections in the first week after injection, and if that wave is excluded from the calculations, then the VE will naturally appear to be higher than it is. Also, as time passes and more breakthrough cases occur, the relative significance of that initial wave will diminish. As a result, the effectiveness of the vaccine will appear to wane. In other words, both the VE figures and their subsequent waning are nothing more nor less than statistical illusions caused by ignoring the initial wave of infections. The possibility of this ‘illusion’ is well established, and has been openly discussed. So serious is this matter that it has the potential to make an entirely useless vaccine, one with a known effectiveness of precisely zero, appear to have a VE of 70% or more.
Mathematically, if the vaccine causes some infections in the first week, if these are ignored, and if the VE wanes down to zero, then by definition the vaccines must have caused more infections than would have been the case without any vaccines.
It is important to remember that the experimental Covid shots were given ‘Emergency Use Authorization’ on the basis of clinical trials that claimed the product prevented symptomatic infections. When these claims proved to be wrong based on real-life observational studies, the rollout of the vaccines should have been halted immediately until randomised control trials were able to establish some other benefit. Instead, the narrative was changed. The new claim was that the vaccines prevented severe disease and death. Multiple studies were published reporting that, despite waning effectiveness in terms of infections, the shots maintained stable VE values for severe Covid and Covid deaths.
Is the new narrative true? It is not. In the first place, all the studies known to us that claim the VE remains stable in terms of severe illness or death have the same inherent flaw mentioned above, namely that vaccinated persons were treated as if they were either unvaccinated or in a ‘control’ group during the week following injection. It is useful to look at a particular study as an example. Johnson et al. concluded that, between October and November 2021, “unvaccinated persons had … 12.7 times the risks for … Covid-19 associated deaths compared with fully vaccinated persons.” Despite such glowing results, however, the authors expressly note that “partially vaccinated persons were excluded.” What this means is that every vaccinated person who died with a positive Covid status was excluded if the specimen used in the test was collected between the date of the first dose and 14 days after the second dose. Since we know that this time window involved two separate spikes in infections (one after each dose), the conclusions of this study are meaningless unless some proof of a massive reduction in infection fatality rate (IFR) during that same period is provided. This they failed to do.
Indeed, a study that followed five million people receiving two doses of the experimental Covid injections found that 96% of Covid deaths (1,950 of 2,031) happened before day 14 after the second dose. This study was not actually trying to calculate VE, but rather the risk of a Covid death after vaccination. They expressly excluded Covid deaths during the 14 days after the first dose: “People entered the cohort at 14 days after their first vaccination dose.” So we do not have a full tally of deaths after dose 1. What is certain, however, is that it is easy to see why ignoring these periods will result in a favourable efficacy score.
Some people might argue that since only 4% of the deaths happened after ‘the vaccines took effect’, this is proof that the shots worked. Is it so? Certainly not, for it is not right to ignore extra infections or deaths solely because they happened shortly after the injection. Further, this study followed people for only 35 days (on average) following the 14 days after the second shot. This is too small a window to affirm anything. Also, and critically, the study period ended on June 15, 2021, a time when the background rate of Covid deaths in England had been almost zero for two whole months.
Second, the calculation of vaccine efficacy in terms of severe disease or death typically involved the use of incorrect or unreliable numbers. As we have already mentioned, randomised controlled trials were done to establish a reduction in infections. They were not done to establish a reduction in severe disease or death. This forced researchers to rely on observational and ‘real world’ data. Even if this data was itself accurate, using it to calculate VE is particularly difficult for various reasons. For instance, it is not easy to determine the number of unvaccinated individuals in a population. While counting the number of vaccinated people is as simple as recording all those who received an injection, counting the people who were never injected is another story altogether. Likewise, a decrease in the background infection rate during the rollout, or rolling out a vaccine over a period of several months, both have the tendency to artificially inflate the VE. Another confounding factor is that the unvaccinated may have been subjected to more testing than the vaccinated, thereby causing an upward bias in the number of Covid cases among the unvaccinated.
Third, we have already established that the Covid shots increased the odds of being infected with Covid. In order for the shots to simultaneously increase infections and prevent deaths it would be necessary for the vaccines to cause a significant drop in the IFR of Covid among the vaccinated. A study by Ophir et al. examined multiple papers for evidence of such a drop, but were unable to find any. They concluded that “the widely accepted medical narrative today, as if the booster doses of the mRNA vaccines prevent severe illness and deaths despite their failure to protect against infections, lacks scientific support.”
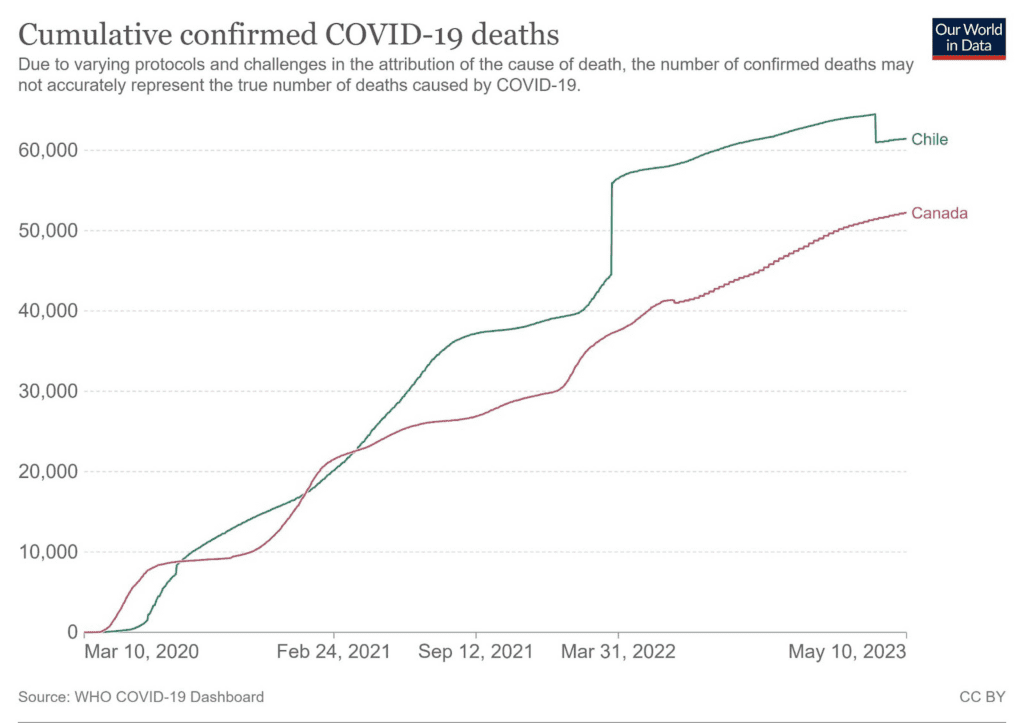
Fourth, deaths attributed to Covid continue to be recorded in highly vaccinated countries at rates similar to what was seen before the injections were rolled out. For instance, a plot of Covid deaths in both Chile and Canada fails to reveal a decline in death rates, but instead shows a fairly consistent slope through 2021 and 2022, despite the high vaccination rates in both countries (Canada: 83%, Chile: 88%, by the end of 2021).
Conclusion
In summary, since we know that the experimental Covid injections increased the rates of infection among the vaccinated, and since there is no scientific evidence of a corresponding reduction in the IFR, in all probability the rollout of the Covid vaccines actually increased the number of Covid deaths. However, to be conservative, to give the shots every possible benefit of the doubt, and because factual and specific data in this regard is lacking in the scientific literature, it is best to say that the injections probably prevented no Covid deaths.
As startling as such a conclusion might be, it bears pointing out that Dr. Fauci himself recently contributed to a paper that rather bluntly observed of vaccines in general, and of the Covid vaccines in particular, that “past unsuccessful attempts to elicit solid protection against mucosal respiratory viruses and to control the deadly outbreaks and pandemics they cause have been a scientific and public health failure that must be urgently addressed.” It is most certainly a “public health failure” when a vaccine is rolled out at enormous cost and injected into billions of arms, and yet prevents no deaths.
To put things into the proper perspective, the strange aspect of the past few years is not that the vaccines were such a dismal failure. Rather, what is odd is that any manufacturer claimed to have developed a vaccine for Covid at all. We are reminded that despite years of research and efforts previous to December 2020, “no effective vaccine has yet been approved for the prevention of human coronavirus infection.” Indeed, as late as June 2020, Moderna published a paper pointing out that “no mRNA drug has been approved in this new potential class of medicines, and may never be approved as a result of efforts by others or us. mRNA drug development has substantial clinical development and regulatory risks due to the novel and unprecedented nature of this new class of medicines.”
The vaccines may have been useless at preventing Covid deaths, but were they entirely harmless? Were there any adverse events from these injections? We have already noted that a significant percentage of people developed Covid-like symptoms. Did anyone die as a result? It is this important matter that we hope to address in the next part of this series.
This article forms part of PANDA’s ongoing inquiry into the drivers of excess deaths. Please consider supporting PANDA’s independent insights with a donation.
As you said "A study done in the UK, and involving more than one million participants, found that an almost unimaginable 33.8% of vaccinees reported Covid-like symptoms in that first week after injection". This to me is preposterous ... unless we believe that Covid was "lying in wait ready to pounce on vaccinees" in the week or so after an injection (that'd be a super smart virus!). I'd suggest an alternative reason: the mRNA/DNA jabs turn people into spike factories, and considering the spike is a major component of the virus (some would say the most important component), if that isn't effectively giving the vaccinees Covid then what is it? So despite the official claims - often repeated - that the jabs "can't give you Covid", I disagree, I'd suggest that's exactly what they do to many people (not all perhaps) and hence why so many people suddenly test + soon after their injections.
Great article --as you say "completely useless"
I would also say "completely unnecessary" bearing in mind the very low if not zero IFR especially for children.